S2E2: Acute Asthma Exacerbation - PHEM
Welcome back to TheCase.Report!
We’re back with our very first PHEM episode, a long overdue milestone.
For the case, Mohammed is joined by Jamie and AP extraordinaire, Joe Mooney.
Our Adult in the Room, Dr Jason van der Velde, then reviews our work and adds some pearls.
Callum is back with The Echo Chamber, where he’s joined by Dr Florian Pracher, who takes us through the use of POCUS in his practice as a retrievalist, and the importance of structured training and accreditation.
Right, let’s get to it!
Asthma
This is common. And no more so than in Ireland! We have one of the highest rates of asthma in the world (Masoli, Matthew, et al. "The global burden of asthma: executive summary of the GINA Dissemination Committee report." Allergy 59.5 (2004): 469-478.)
Just under half a million people in Ireland have asthma.

4th highest prevalence in the world

It’s costly, and again… COMMON!

So we’ve about 50 annual deaths from asthma, compared to 200 in the UK, but that means we have a 3 times higher rate of death from asthma here! Why is that?
People don’t tend to get suddenly extremely ill and die from asthma out of nowhere. Some do get sudden severe exacerbations out of nowhere it’s true, but most are chronically poorly controlled. So is our excess asthma mortality a psychosocial issue? A consequence of poor access to primary care? Fewer GP contacts a risk factor for developing fatal/near-fatal asthma, and lack of a single payer universal health system has demonstrable effects on GP attendance (https://www.tandfonline.com/doi/full/10.1080/13814780701815082?src=recsys)
Lots of inequities in our current system may be playing a role (https://www.tandfonline.com/doi/full/10.1080/23288604.2018.1551700)

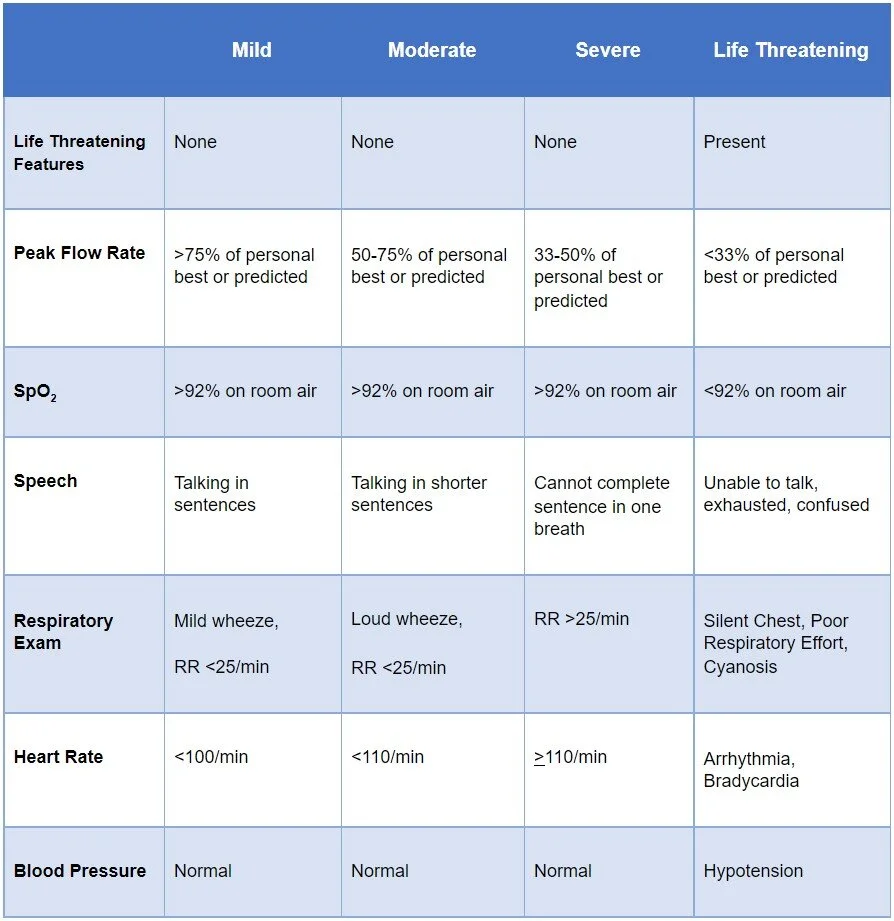
Early care, recognition of the critically unwell asthmatic - risk stratification - BTS Guidelines for severe, life threatening etc. (Table below).
So like we talked about earlier in the case, recognition of what we’re dealing with is key. Talk us through what differentiates our levels of exacerbation.
What helps you differentiate between them?
Indicators of Life Threatening Asthma on Arterial Blood Gas sampling include:
· PaO2 <8.0kPa
· PaCO2 normal
o With tachypnoea, CO2 is being expired much more quickly and as such should be low on an ABG. A normal or raised PaCO2 indicates the patient is tiring and moving less air.
An exacerbation of asthma that requires mechanical ventilation or presents with a raised PaCO2 is defined as near fatal.

So where do we start in terms of treatment?
Oxygen if they’re hypoxaemic
Controlled supplementary oxygen to all hypoxaemic patients with acute severe asthma titrated to maintain an SpO2 level of 94–98%.
β2 agonist bronchodilators
Mild/moderate can use metred dose inhaler and spacer.
Oxygen driven nebs otherwise
Consider continuous nebs if not responsive to initial therapy
IV if all else fails, but monitor lactate
Steroids
40-50mg prednisolone PO or 100mg hydrocortisone IV
As effective as higher doses
Ipratropium Bromide
Adding ipratropium (0.5mg) to β2 agonist produces greater bronchodilation than β2 agonist alone
Magnesium Sulphate
Ooof… anecdotally amazing, but…
Long story short, single dose of 2g IV over 20mins
Systematic review of 25 RCTs - no benefit in lung function/need for admission (caveat, normal drawbacks of meta analyses and SRs)
Some modest improvements in lung function and reduce intubation rates in other studies.
Aminophylline
Like, I guess we’ll think about it, but then more than likely not give it.
5mg/kg loading dose over 20 minutes (unless on maintenance oral therapy) then infusion of 0.5–0.7 mg/kg/hr
Risk of arrhythmias with no likely additional bronchodilation? Sounds like a bad deal
Other therapies we won’t be doing
IVF and IVAbx unless specifically indicated, leukotriene receptor antagonists (LTRAs), Heliox, nebulised furosemide
NIV
Before we begin discussing NIV, there are 2 important caveats:
It’s important to note that if we don’t have a patient that is improving in front of us at this point, after all the above intervention, we need to be speaking to our critical care colleagues, because whatever else happens, they will need to be involved.
If we’re seeing a patient who is ticking the boxes for intubation and mechanical ventilation, do not use NIV to delay the inevitable.
Now onto NIV. It’s used not uncommonly for acute severe asthma in different parts of the world, but not commonly around these parts.
Several studies done including a Cochrane review have been inconclusive, and have had small sample sizes. The issue is that exacerbations rarely progress to the point where intubation is required so it’d be difficult to recruit large numbers for an RCT.
Some others have shown benefits in terms of reduced hospital and ICU stays.
But how would NIV help?
Let’s talk about how work of breathing gets trickier in exacerbations:
Bronchoconstriction and secretions result in expiratory airflow limitation.
Delayed emptying with incomplete expiratory phase interrupted by next inspiration starts to hyperinflate the lung, increasing intrinsic PEEP (iPEEP/auto-PEEP)
Increased intrathoracic pressure means patient has to generate EXTRA negative pressure to move air in with next inspiration, so extra work for those inspiratory muscles
Expanded chest wall means inspiratory muscles are at a disadvantage in terms of their length-tension curves AND have to work harder than usual
Breathing is happening in the less compliant upper part of the pressure-volume curve

That is a lot of hard work! And now you can understand how these patients can tire rather quickly.
So where does NIV come in? How can it help?
This is still a challenging concept, and it is completely paradoxical on the face of it: overcoming intrinsic PEEP by applying extrinsic PEEP
Low levels of extrinsic PEEP can reduce that pressure gradient between distal and central airways, and maybe the iPEEP as well, reducing the required intrathoracic pressure to initiate a breath, and offloading the work on the inspiratory muscles.
Caveat here is that ePEEP should not exceed iPEEP, but unlike the expiratory hold in intubated patients, there’s no way of measuring iPEEP in patients who are self ventilating.
Where do I come down on this? Well if this is part of your practice already, I’d love to hear from you about your experience…
If you’re like me and it’s not, then I don’t know if I’m swayed enough by the evidence out there to change my ways. If we were to see studies showing it to be safe and effective at reducing intubation then I’d be delighted, but at the moment I’d just be afraid we’re delaying intubation and possibly causing harm.
RSI and mechanical ventilation
Recognising that intubation doesn’t solve the problem but helps facilitate you solving the problem in a more organised fashion. Don’t be tempted to feel accomplished and step back once the tube is in and air is moving, the battle to ventilate has only really begun at that stage.
Indications:
arrest
severe hypoxia
altered mental state
failure to respond to treatment
How we go about it:
Drugs: Ketamine ideally (bronchodilation effect); emergency vasopressors; rocuronium
Tube: Go big (bigger lumen, lower airway pressure: Hagen-Poiseuille if you remember it)
Fluids
Checklist: Always checklist, and use one specifically made with COVID in mind
Very gentle hand ventilation until ventilator is set up
Ventilator setting principles:
TV ≤6ml/kg
I:E ratio ≤ 1:4
Pplat ≤25cmH2O
PEEP: 60-80% iPEEP
Possible complications:
Hypotension:
sedation, hyperinflation, tension pneumothorax, arrhythmias, hypovolaemia (rare), endobronchial intubation, myocardial depression from prolonged hypoxia, reversal of pleural pressures impairing venous return
Pneumothorax:
Urgently decompress if signs of tension
Arrest:
Usual ALS principles, but with above considerations and manual decompression if dynamic hyperinflation suspected
VV ECMO
Won’t be starting this in the ED, so won’t dwell on it.
Can improve survival in near fatal asthma by enabling good gas exchange without aggressive ventilation, avoiding barotrauma.
Not widespread in Ireland... yet.
https://www.sign.ac.uk/sign-158-british-guideline-on-the-management-of-asthma
Brenner B, Corbridge T, Kazzi A. Intubation and Mechanical Ventilation of the Asthmatic Patient in Respiratory Failure. Proc Am Thorac Soc . 2009. 6;371-379
Is your management different to ours? Let us know what you’d do differently, or any useful pearls you’ve picked up along the way.